It's often possible to keep training with sore muscles, but it isn't always the smart choice. The key question isn't whether you train at all. It's whether your pain pattern, movement quality, and overall load suggest keeping the stimulus, modifying it, or taking a pause.
Key takeaways
1. Mild: keep training, but modify it.
2. Moderate: shift the focus or train a different system.
3. Severe or unusual: rest or choose active recovery.
Muscle soreness is often not a stop sign, but a signal about tissue tolerance, training novelty, and recovery. If you're trying to balance performance, daily life, and long-term health, a clear decision framework is more useful than blanket rules like "always push through" or "always rest."
This article shows you how to tell typical muscle soreness from warning signs, how to adjust intensity, volume, and exercise selection, and which markers you can check in under a minute. The goal isn't toughness for its own sake, but consistency without unnecessary escalation.
Where Muscle Soreness Fits into the Bigger Picture
Muscle soreness sits at the intersection of recovery and the musculoskeletal system. It tells you something about how your tissues responded to a training stimulus, especially if the load was new, the eccentric demand was high, or your sleep, stress, and training structure aren't lining up well right now. In practice, that means soreness is feedback, but not a clean marker of progress.
If you want to stay fit, capable, and high-performing over the long term, it helps to think about training stimulus and recovery together. That's why, with DOMS, it's worth looking beyond the sore muscle itself and checking sleep, stress, and whether your current training week calls for adjustment rather than escalation. If you want a better sense of the factors that shape recovery, this overview of Sleep & Recovery – Overview can help.
Quick Answer
With mild muscle soreness, you can usually keep training if you reduce intensity and volume, warm up thoroughly, and choose work that promotes blood flow rather than further damage. Hard eccentric loading and sets pushed close to your absolute limit are often the worst combination for the exact muscle that's already sore. If movement quality, range of motion, and strength feel clearly better during the warm-up, that points more toward modified training. If the pain is unusually severe, sharp, accompanied by swelling, or clearly affects function, rest or alternative training makes more sense. If you have dark urine, pronounced weakness, feel unwell, or have very severe symptoms, get medical advice.
- Mild: keep training, but modify it.
- Moderate: shift the focus or train a different system.
- Severe or unusual: rest or choose active recovery.
- Red flags: don't keep training; get it checked.
If you don't want to make this call by feel every time, you can log your 60-second readiness check in the huuman app and see how pain, sleep, and movement quality interact.
The 60-Second Readiness Check with Decision Tree
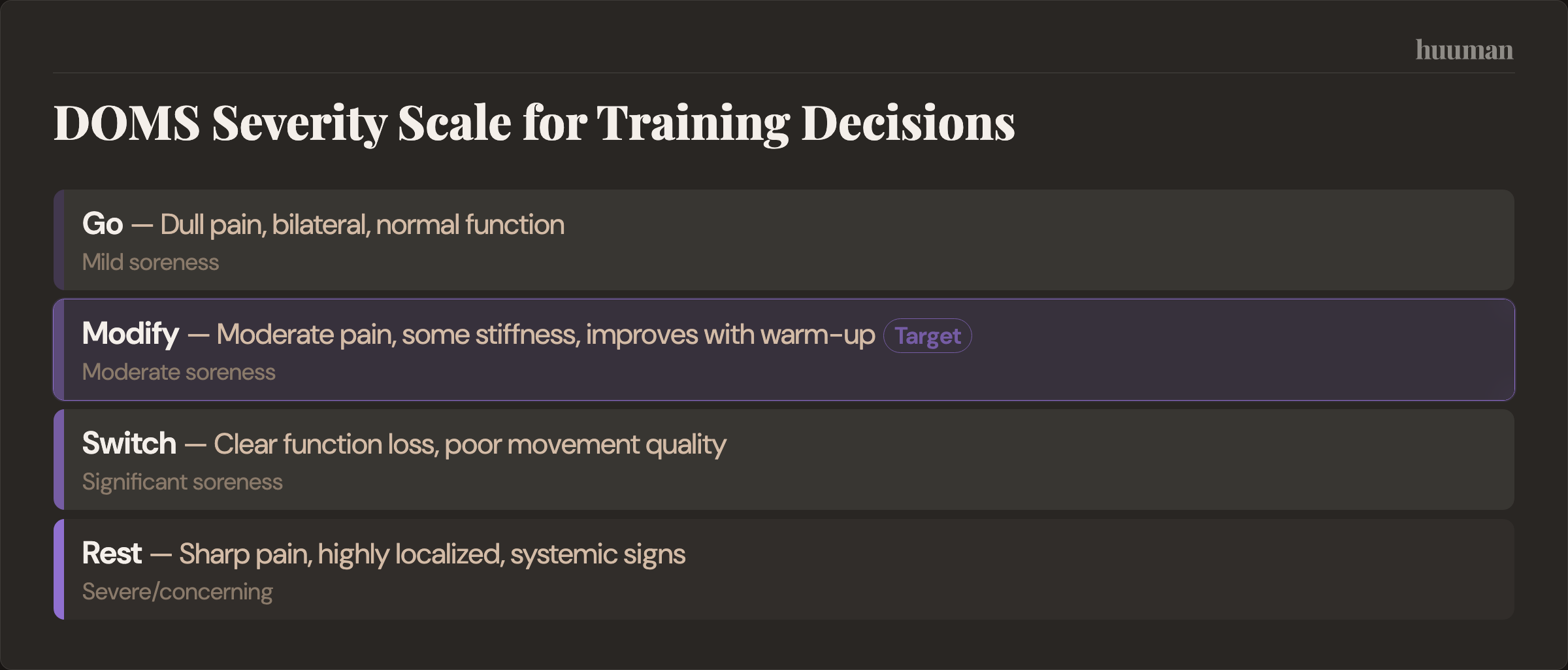
The biggest mistake with muscle soreness is judging only pain intensity. To make a useful decision, you need four layers: pain quality, function, response to warm-up, and systemic signs. That's the logic behind Go, Modify, Switch, or Rest.
60-Second Checklist
- How it feels: Is the pain dull, tender to pressure, delayed after training, and often on both sides? That fits DOMS more closely. Is it sharp, sudden, highly localized, or tied to a clear "pull" in one structure? Be more cautious.
- Function: Can you perform the basic movement cleanly without compensation? Depending on your training, check an air squat, hip hinge, pressing, pulling, or an overhead reach.
- Warm-up trend: Does it loosen up and feel more coordinated after a few minutes? That supports modified training. Does it get sharper, less stable, or more restricted? That's a warning sign.
- System: Do you feel ill, feverish, unusually fatigued, or have marked swelling, visible bruising, dark urine, or clear weakness? Don't normalize it. Stop and get it checked.
Decision Tree: Go, Modify, Switch, Rest
- Go: typical mild muscle soreness, stable movement quality, warm-up improves how it feels, no systemic warning signs.
- Modify: typical muscle soreness, but ROM, coordination, or load tolerance are limited. You still train, but reduce the aggravating variables.
- Switch: the affected muscle is too limited for quality training, but other muscle groups or easy cardio are no problem.
- Rest: unusual pain, a clear functional issue, or systemic red flags. In that case, rest or medical evaluation is the better choice.
What Muscle Soreness Is, and What It Isn't
Muscle soreness, or DOMS, is delayed-onset muscle pain after training. A typical pattern is that it doesn't hit suddenly during the workout, but becomes noticeable hours later, is tender when you press on the muscle, and often affects both sides similarly if the stimulus was symmetrical. DOMS commonly appears as a response to unaccustomed exercise. So treat that as a solid practical guideline rather than an exact timetable for every person.

What does not fit typical DOMS is sharp pain, a clear pain point, a sudden event during a rep, visible bruising, instability, or an obvious loss of strength in the movement. That points more toward a strain, overload reaction, or another injury. In practice, that distinction matters more than arguing about whether training with soreness is "allowed."
Why DOMS Happens, and Why Repeated Exposure Often Feels Easier
DOMS is likely linked to exercise-induced changes in muscle tissue, a follow-up inflammatory response, and increased tissue sensitivity. Eccentric loading is a particularly strong trigger. One systematic review describes eccentric exercise as being associated with muscle fiber injury, strength loss, soreness, and altered membrane permeability, with inflammation playing a role in recovery during eccentric exercise.
That helps explain why new exercises, slow lowering phases, lots of loaded stretch positions, downhill running, or sudden jumps in volume often create more soreness than familiar, technically controlled work. It also explains why DOMS is not automatically a sign of a "better" session. It usually tells you the stimulus was new or relatively high for your tissues.
One important concept here is the repeated bout effect. After an initial unfamiliar eccentric stimulus, muscles often respond to a similar bout later on with less damage and less soreness. A PubMed-listed paper describes this adaptation after eccentric loading as protection during subsequent exposure. In practice, that means the first exposure in a new training phase is often the roughest. Consistency beats surprise.
What Happens If You Train Despite Muscle Soreness?
Usually, nothing dramatic happens automatically. The more realistic issue is that performance, coordination, and range of motion may be temporarily worse. DOMS can affect athletic performance by causing a reduction in joint range of motion, shock attenuation, and peak torque. Alterations in muscle sequencing and recruitment patterns may also occur, causing unaccustomed stress to be placed on muscle ligaments and tendons.
So the better question is not "Am I allowed to train?" but "Can I do a useful version of this session today?" If you can't control depth in your squats, lose position during pulling movements, or every lowering phase in the sore muscle feels unnecessarily brutal, the answer isn't more willpower. It's better exercise selection.
The same logic applies to endurance training. Leg DOMS may still allow easy cycling or light running, while downhills, sprints, hard intervals, or plyometrics may be a poor fit because they reintroduce high eccentric stress or reduce landing control.
How to Adjust Training with DOMS
If you want to keep training with sore muscles, six levers matter most: intensity, volume, exercise selection, tempo, range of motion, and proximity to failure. In training practice, these are exactly the variables used to make loading more tissue-friendly without skipping training entirely.

DOMS Adjusters: A Quick Cheat Sheet
- Intensity: Choose loads you can move with clean technique. More reps in reserve and no grinding are usually smarter than sets pushed near your max.
- Volume: Cut sets or exercise count before you cut the warm-up. With DOMS, a short high-quality session is often better than a full program done badly.
- Exercise selection: Favor more stable options if coordination is off. Machines, guided patterns, or less complex variations can be more helpful temporarily than free weights with high technical demand.
- Tempo: Dial down the eccentric phase. Slow negatives, jumps, or heavily loaded stretch positions are often the wrong lever here.
- ROM: Use the pain-free or well-controlled range. Deep loaded stretch positions are not automatically brave; they're often just more irritating.
- Proximity to failure: Keep some distance from your limit. If RPE rises and technique falls apart at the same time, the session quickly becomes extra fatigue instead of productive training.
Examples by Situation
- Mild leg soreness: easy cycling, technical practice, moderate leg press, controlled split squats to a well-controlled depth instead of heavy squats with a long eccentric phase.
- Moderate leg soreness: train upper body, do easy zone 1 to 2 cardio, mobility, and light pump work instead of intervals, hill running, or downhills.
- Upper-body soreness: train lower body or do easy endurance work, simplify pressing or pulling patterns if needed, and avoid deep loaded stretch positions such as dips or flyes.
- Returning after a break: don't stop training completely, but use repeatable, moderate sessions instead. If you want a more structured approach to temporarily reducing load, topics like deloads, how long to deload, how often to deload, deloads in bodybuilding, and a sample deload week may also be useful.
Active Recovery: What's Actually Realistic?
Active recovery can help reduce the sensation of soreness in the short term and make movement feel better again. That does not mean the tissue is somehow magically "repaired." In practice, the usual options are easy zone 1 to 2 cardio, light mobility work, and light pump-style training, as long as they reduce symptoms rather than aggravate them.
A systematic review with meta-analysis on recovery techniques evaluated different methods for reducing muscle soreness, fatigue, and inflammatory markers across different recovery methods. The general direction of the evidence suggests some strategies may have small to moderate effects, but the results are not uniform and do not work the same way for everyone. For massage, a separate systematic review and meta-analysis also found effects on recovery, though again without any guarantee or universal superiority.
That makes the practical priority clear: first adjust the training intelligently, then use simple recovery measures. For many people, sleep, adequate protein intake, hydration, and stress management matter more for the overall picture than chasing the perfect recovery hack. If sleep is an issue, waking in the middle of the night may also be relevant, since broken sleep often makes recovery harder to manage.
Evidence and Limitations
Research supports several points reasonably well: DOMS typically shows up after unfamiliar loading, eccentric work is a common trigger, and the repeated bout effect is well described. There are also systematic reviews and meta-analyses on recovery strategies such as massage and other methods, suggesting small to moderate effects.
The evidence is weaker when it comes to questions like how many rest days are "right" or which universal rule works across all training styles. That's exactly why rigid calendar rules rarely work well. Muscle soreness is a fuzzy marker. Two people with similar pain may differ a lot in actual function. That's why movement quality, warm-up response, and overall state are usually better decision tools.
For light movement as a short-term way to ease DOMS, the literature is fairly encouraging in practice, but the sources provided here do not cover it directly enough to justify a strong standalone claim. The same applies to specific pain-scale thresholds or exact timelines for full readiness again. Careful interpretation is more honest than false precision.
When red flags for rhabdomyolysis are present, clinical caution matters, but the specific studies provided do not directly cover that point. So the guidance here is intentionally conservative: very severe muscle pain after extreme unfamiliar exertion, pronounced weakness, dark urine, fever, or a clear sense of feeling unwell are not signs of a normal "hard session." They are reasons to seek prompt medical assessment.
Strategies to Discuss with a Professional
If your soreness is mild, there is often a strong case for the "Modify" approach. The goal is blood flow, technique, and a moderate stimulus, not destruction. Many programs do this with lower loads, less volume, simpler variations, and a less aggressive eccentric phase.
If soreness is moderate and function is clearly affected, "Switch" is often the better solution. Train other muscle groups or another energy system. Upper body instead of legs, easy cardio instead of intervals, technique instead of performance. That keeps the habit intact without overloading the same irritable area again.
If symptoms are severe or unusual, "Rest" or very light active recovery is often the smartest option. Daily movement, gentle mobility, sleep, and better load management are usually more useful than forcing a poor session. If it feels like fatigue and stress are building not just locally in the muscles but systemically, Mental Overload: Recognizing the Symptoms, Understanding the Causes, and Lightening Your Mental Load may also be a relevant part of the picture.
For busy professionals training twice a week, a minimum-effective-dose approach can work well. One common setup is one full-body day with a normal stimulus when you feel fresh, and a second lighter or more technical day. If DOMS is high, that second session may become easy movement plus mobility instead of another hard stimulus. That logic is often more sustainable than constantly flipping between all-out effort and complete rest.
Nutrition and recovery also deserve context. If training temporarily changes your appetite, that can affect your day-to-day recovery, similar to what's described in does strength training make you hungrier than cardio? And if fatigue stays high despite caffeine, it may be worth looking at why caffeine can make you feel tired, since feeling alert and actually being recovered are not the same thing.
How to Measure and Interpret Progress
The best protection against poor decisions is simple tracking. You don't need complicated tools. Four markers are enough: pain quality, function, warm-up trend, and overall system state.
The Four Markers
- Pain: Note whether it's dull or sharp, improving or worsening, bilateral or highly localized. Dull, bilateral soreness that improves with movement is typical DOMS. Sharp, one-sided pain that worsens with movement suggests injury.
- Function: Test one or two quick screens like an air squat, hip hinge, or overhead reach. Focus on movement quality, not depth. Can you move smoothly without compensation patterns?
- Performance: Track how your warm-up feels. Does movement become more fluid after 5-10 minutes? Does technique stay stable under light load? If warm-ups consistently feel heavy or technique breaks down early, that's a clear signal to modify.
- System: Monitor sleep quality, subjective fatigue, stress levels, and if available, resting heart rate or HRV trends. Look at patterns across several days, not single readings.
Record these markers daily during recovery periods. Note which muscle groups are affected, pain intensity (1-10), movement quality during your function check, and how you responded to warm-up. Add sleep hours, stress level, and what training decision you made.
After a week, patterns emerge. You might notice that poor sleep consistently makes soreness last longer, or that certain exercises always need extra recovery time. You might find that moderate movement on day two speeds recovery, while complete rest actually prolongs stiffness.
If you want to turn these observations into actionable patterns, you can track your recovery signals and training sessions in the huuman app to identify when modifying works better than pushing through.
Signal vs. Noise in Muscle Soreness
- Signal: soreness after a new exercise or unusually high eccentric work makes sense. Next time, don't just check the soreness; look at whether you can build the stimulus more gradually.
- Signal: movement quality breaks down even though motivation is there. Change the exercise or the range of motion first, instead of simply trying to push harder mentally.
- Signal: the pain gets worse during the warm-up instead of better. Shift the focus of the session and see whether alternative training is problem-free.
- Signal: pain at rest, clear swelling, or visible bruising do not fit normal DOMS well. Get it assessed professionally.
- Signal: very severe muscle pain, weakness, and dark urine after extreme exertion are not a normal recovery issue. Seek medical assessment quickly.
- Noise: "No soreness, no progress." Progress depends on repeatable quality and total training load. Bring your focus back to performance, technique, and consistency.
- Noise: "Stretching cures soreness." Gentle mobility can feel good, but it's not a reliable repair button. Watch how you respond over the course of the day.
- Noise: "Ice baths are always better." Some methods help some people, but effects vary. Only keep what actually makes your training easier to manage.
- Noise: "You have to push through the pain." What matters is not toughness, but whether you can still control the basic movement cleanly. If you can't, change the plan.
Frequently Asked Questions
What happens if you train with sore muscles?
Usually, movement quality, strength perception, and coordination drop temporarily. The main issue is often not the soreness itself, but the lower quality of execution. DOMS can affect athletic performance by causing a reduction in joint range of motion, shock attenuation, and peak torque. If you adjust the session, continuing to train can make sense. If you load the same structure hard again, especially with high eccentric stress, you are more likely to create unnecessary irritation.
How long should you wait to train after muscle soreness?
There is no clean universal rule. More important than counting days is whether function comes back, the warm-up improves the situation, and no warning signs are present. Mild DOMS often does not mean you need to rest. Severe or unusual pain points more toward rest or alternative training.
Does muscle soreness mean you trained properly?
Not necessarily. Muscle soreness mainly tells you the stimulus was unfamiliar or relatively high. You can make great progress with very little DOMS, and you can have lots of DOMS without especially effective training. What matters is repeatable performance, technique, and recovery.
Can I jog or cycle with sore muscles?
Often yes, as long as it stays easy and your technique does not fall apart. With leg DOMS, cycling is often easier to control than downhill running, sprinting, or interval work. If the movement makes things feel better, that is usually a good sign. If it makes things worse, change the plan.
What helps muscle soreness quickly?
Some people get short-term relief from easy movement, massage, or other simple recovery strategies. The evidence points more toward small to moderate effects than anything dramatic. In most cases, good load management, sleep, protein intake, and hydration are more reliable than aggressive recovery hacks. If you're looking for more day-to-day biomechanical relief, some people also look at things like the best recovery sandals in detail, though that doesn't automatically make training itself better managed.
Should I train the same muscle again or switch to a different muscle group?
With mild, typical DOMS, the same muscle can often still be trained in a modified way. With moderate DOMS, switching to other muscle groups or to easy cardio is often the better option. If you notice compensation patterns, a major loss of ROM, or sloppy technique, switching is usually the smarter decision.
When is muscle soreness not normal and a reason to see a doctor?
If the pain is sharp, sudden, or very localized, or if it comes with obvious swelling, bruising, marked weakness, pain at rest, fever, feeling unwell, or dark urine, you should get it medically assessed. That is especially true after extreme unfamiliar exertion or if symptoms are getting worse rather than fading.
If you don't want to improvise these decisions every session, your huuman Coach can adjust weekly plans and interpret your recovery data in context so training load, sleep, and exercise selection work better together.
More health topics to explore
- Sleep & Recovery – Overview
- Sleep Duration at Age 3: Guidelines, Naps & a Practical Reality Check
- How Often to Deload: Frequency, Triggers, and 3 Deload Week Templates
- Deep Sleep Pillow Spray: What It Is, Whether It Works, and How to Choose Safely
References
- Bennett M et al. — Hyperbaric oxygen therapy for delayed onset muscle soreness and closed soft t... (2005)
- Daniel Vasile PR et al. — Evaluation of curcumin intake in reducing exercise-induced muscle damage in a... (2024)
- Howatson G et al. — Repeated bout effect after maximal eccentric exercise (2007)
- Dupuy O et al. — An Evidence-Based Approach for Choosing Post-exercise Recovery Techniques to ... (2018)
- Davis HL et al. — Effect of sports massage on performance and recovery: a systematic review and... (2020)
- Hotfiel T et al. — Advances in Delayed-Onset Muscle Soreness (DOMS): Part I: Pathogenesis and Di... (2018)
- Borghi SM et al. — Intense Acute Swimming Induces Delayed-Onset Muscle Soreness Dependent on Spi... (2021)
- Physio-pedia — Delayed Onset Muscle Soreness