Intermittent hypoxia is gaining attention because it sits at the intersection of endurance training, respiratory physiology, metabolic health, and recovery. The idea is simple: expose the body to brief periods of lower oxygen, then return to normal air, using the change as a controlled stressor.
Key takeaways
1. Best simple definition: intermittent hypoxia means alternating between hypoxia, lower-than-normal oxygen exposure, and normoxia, normal air recovery.
2. Training use: intermittent hypoxic training, or IHT, usually combines lower oxygen exposure with exercise or structured breathing through a device.
3. Conditioning use: intermittent hypoxia conditioning, or IHC, usually refers to repeated hypoxic exposures designed as a conditioning stimulus, often without hard exercise.
The important word is controlled. Repeated oxygen drops can be adaptive in some supervised settings, but they can also be harmful when they occur in the wrong context, especially during obstructive sleep apnea. The same broad term can describe a research tool, an athletic training method, a clinic-based intervention, or an unsafe nightly exposure.
This guide explains what intermittent hypoxia means, how it differs from altitude training and breath-holding, what mechanisms are plausible, where the evidence is limited, and how a conservative at-home structure is commonly described. It is not a treatment plan, and it is not a reason to ignore medical risk factors.
Where intermittent hypoxia fits in health and performance
Intermittent hypoxia belongs in the same category as heat exposure, interval training, fasting, and other stress-based interventions: the intended benefit depends on matching the stress to the person’s current capacity. Too little may do nothing meaningful. Too much may create headache and other hypoxemia symptoms, excessive sympathetic activation, and blood pressure strain, and some people also report disrupted sleep or anxiety-like feelings.
For heart and cardio health, the main questions are vascular tone, autonomic balance, blood pressure response, and the crucial distinction between intentional short exposures and uncontrolled oxygen drops during sleep. If you are building the basics first, the broader Heart & Cardio foundation matters more than any hypoxia device.
For metabolism, intermittent hypoxia is often discussed as a cellular signaling stressor that may influence mitochondrial function, glucose handling, and fuel use. Those claims are biologically plausible, but they should not be treated as guaranteed outcomes. Training consistency, sleep, nutrition, body composition, and recovery still dominate the signal.
For recovery, hypoxia is not a recovery tool just because it is passive or low impact. It is still a stressor. A seated hypoxia session may feel easier than intervals, but the body still has to respond to lower oxygen, sympathetic arousal, and altered breathing. The useful question is not “Can I tolerate it today?” but “Does this improve the next week of training, sleep, and readiness?”
Quick answer
Intermittent hypoxia is a pattern of brief, repeated exposures to lower oxygen separated by normal-air recovery. In research and some clinical environments, the dose matters: how low the oxygen is, how long each exposure lasts, how often sessions are repeated, and how well the person recovers between them.
- Best simple definition: intermittent hypoxia means alternating between hypoxia, lower-than-normal oxygen exposure, and normoxia, normal air recovery.
- Training use: intermittent hypoxic training, or IHT, usually combines lower oxygen exposure with exercise or structured breathing through a device.
- Conditioning use: intermittent hypoxia conditioning, or IHC, usually refers to repeated hypoxic exposures designed as a conditioning stimulus, often without hard exercise.
- Hyperoxic variation: intermittent hypoxic-hyperoxic training, or IHHT, alternates hypoxia with hyperoxia, higher-than-normal oxygen, but the evidence is mixed and protocols vary widely.
- Who may consider it: healthy adults with strong training and sleep habits who want to test a marginal stressor conservatively, especially endurance athletes or busy professionals seeking low-impact conditioning.
- Who should get medical input first: if you have suspected sleep apnea, heart or lung disease, uncontrolled blood pressure, an arrhythmia history, pregnancy, a seizure disorder, prior stroke, anemia or iron deficiency, or high panic susceptibility, it is safer to talk with a qualified clinician before trying it.
- What to track: symptoms, RPE, lowest observed SpO2 if measured, resting heart rate, HRV trend, blood pressure if relevant, sleep, and next-day fatigue.
If you want clean data before changing the stress, log sleep, sessions, and readiness signals in the huuman app so the pattern is visible beyond one exciting or uncomfortable.
What intermittent hypoxia actually means
Normoxia means normal oxygen availability. Hypoxia means reduced oxygen availability. Hyperoxia means higher-than-normal oxygen availability. In device-based intermittent hypoxia, oxygen exposure is usually manipulated by changing the inspired oxygen fraction, often described as FiO2, or by simulating an equivalent altitude. Without high-quality device controls and appropriate monitoring, those numbers are easy to misunderstand.

Intermittent hypoxia is different from continuous altitude exposure. Spending days at altitude changes the whole environment for sleep, daily movement, training, appetite, hydration, and recovery. An intermittent session compresses the exposure into repeated blocks, often while seated or doing easy aerobic work. That makes it easier to control, but it also means you should not assume it produces the same adaptations as living or training.
Breath-holding is also not equivalent. Breath-holds involve rising carbon dioxide, voluntary suppression of breathing, technique-dependent strain, and higher safety risk, especially in water or while exercising. Device-based normobaric hypoxia changes the oxygen content of inspired air while breathing continues. Both can create air hunger, but they are not interchangeable methods.
Altitude tents and rooms aim to create longer normobaric hypoxia exposures. Hypobaric altitude, such as travel to mountains, changes barometric pressure rather than just the oxygen mixture. Hypoxicators and masks are typically used for shorter, more controlled sessions. IHHT adds hyperoxic recovery segments, but “more complex” does not automatically mean “better.”
The dose principle: the signal or the harm
The key decision framework is simple: the dose determines whether intermittent hypoxia is a manageable training signal or a poorly timed stressor. A conservative dose can be understood through five practical variables: depth, duration, density, progression, and defense.

- Depth: how low the oxygen exposure is, described as FiO2 or equivalent altitude. Deeper hypoxia is not automatically more effective and may increase symptoms.
- Duration: how long each hypoxic interval lasts and how much total hypoxic time occurs in the session.
- Density: how many cycles occur in a session, how many sessions are performed weekly, and how long the program continues.
- Progression: whether only one variable changes at a time or whether oxygen depth, interval length, and weekly frequency all rise together.
- Defense: the person’s recovery capacity, including sleep, HRV trend, resting heart rate, illness, soreness, stress, alcohol, and training load.
The mistake is treating SpO2 like a leaderboard. A lower oxygen saturation reading may indicate a stronger exposure, but it does not prove a better adaptation. It may simply mean the session is outpacing your current tolerance. In practice, the better question is whether the exposure is repeatable without next-day cost.
Monitoring saturation directly adds a guardrail: many clinical references describe an SpO2 below 90% as hypoxemia, a low-saturation level that is a sensible cue to end the session rather than push further.
O2 dose dial table
This is a practical planning table, not a prescription. The goal is to make each decision visible before intensity creeps upward.
- Oxygen depth: Start with mild device settings or supervised defaults rather than chasing deep hypoxia. Do not use specific FiO2 or altitude targets unless the device, clinician, or qualified professional provides validated guidance.
- Interval length: Short exposures give you time to evaluate symptoms and recovery. Longer intervals should only be considered after repeated uneventful sessions.
- Cycle count: Fewer cycles reduce total stress. Adding cycles increases density even if the oxygen setting stays unchanged.
- Total session duration: A 10 to 15 minute microdose and a 50 minute aerobic session are different training stresses, even if both feel “easy.”
- Weekly frequency: Many conservative structures use 1 to 2 weekly sessions as an initial ceiling, especially when the person is already training. Treat added frequency as a progression, not a default.
- Program length: A short exploratory block is mainly about tolerability and pattern recognition. Longer blocks need more careful review of sleep, training quality, blood pressure, and symptoms.
- Deloading: If life stress, poor sleep, heavy training, or illness rises, reduce hypoxic exposure rather than adding more stimulus.
Mechanisms without the hype
The most discussed pathway is hypoxia-inducible factor signaling, often shortened to the HIF pathway. At a high level, HIF-related signaling helps cells respond to lower oxygen availability. It can influence oxygen transport, energy metabolism, vascular signaling, and stress-response pathways. That does not mean every home session creates meaningful adaptation, and it does not mean more hypoxia is better.
Ventilatory acclimatization is another plausible mechanism. Repeated exposure to lower oxygen can change breathing drive and the perception of respiratory effort. For an endurance-trained person, that may feel like improved tolerance during harder aerobic work. For someone prone to panic, air hunger may be destabilizing rather than useful.
Sympathetic activation is part of the stimulus. Lower oxygen increases sympathetic nervous system activity, which can raise arousal and heart rate. That is one reason some people feel alert after a session. It is also why poor timing can disturb sleep or add strain on a day that already includes hard training, caffeine, work stress, and inadequate recovery.
Oxidative stress signaling is often misunderstood. Small stress signals can contribute to adaptation, while large or poorly recovered stress can become harmful. Intermittent hypoxia sits on that edge. A productive exposure should leave the next day intact. If sleep worsens, resting heart rate rises, or readiness falls, the stress budget is already speaking.
Longer-term adaptations such as erythropoiesis, increased red blood cell production, are sometimes discussed in the context of altitude and hypoxia. Whether a short intermittent protocol meaningfully affects oxygen-carrying capacity depends on the protocol, baseline status, iron availability, training history, and duration of exposure. It should not be assumed from a handful of sessions.
Potential benefits, interpreted carefully
Endurance athletes usually care about whether intermittent hypoxia improves tolerance to intensity, perceived breathing control, or training adaptation. It may be most relevant for people who already have structured aerobic work in place, including easy volume and intervals. If your base is inconsistent, improving ordinary aerobic training is likely higher leverage than adding a specialized stressor. Practical options like cycling zone 2, zwift zone 2 training explained, and all about 45 minute treadmill workout are often simpler starting points.
The zone boundary matters. Hypoxia can push a session that looks easy on the outside into a harder internal load. If the goal is aerobic development, understanding zone 2 vs zone 3 training may prevent the common mistake of turning every hypoxic block into threshold work.
Strength and functional trainees may be interested in cardiometabolic benefits without more impact. In that case, low-impact aerobic pairing is more logical than adding hypoxia to heavy lifting days. People using strength training for weight loss explained or trying to reduce body fat for women should treat hypoxia as optional and secondary to training consistency, energy intake, sleep, and recovery.
Some clinical and rehabilitation research explores intermittent hypoxia in areas such as neurological recovery, cardiopulmonary conditions, or mobility limitations. Those settings are not the same as at-home experimentation. Clinical populations need supervised protocols, medical screening, and clear stop criteria. It would be inappropriate to translate those contexts into a generic wellness routine.
Cognitive, sleep, blood pressure, HRV, and metabolic flexibility claims should be interpreted cautiously. Some people may feel sharper after a mild session; others may feel wired, tired, headachy, or sleep-disrupted. HRV may rise after a well-timed easy block or fall after an excessive one. These are individual response patterns, not proof that the method is universally beneficial.
Risks, screening, and when not to experiment
Obstructive sleep apnea is the most important distinction. OSA-related intermittent hypoxia is not a wellness practice. It is typically paired with sleep fragmentation, repeated desaturation, sympathetic activation, and cardiometabolic strain. Using intentional intermittent hypoxia to “train” your way out of suspected OSA is the wrong interpretation.
Do not DIY intermittent hypoxia without clinician input if you have suspected or known obstructive sleep apnea, uncontrolled high blood pressure, arrhythmia history, heart disease, lung disease, prior stroke, pregnancy, seizure disorder, anemia or iron deficiency, severe anxiety or panic susceptibility, or unexplained shortness of breath. These are not minor footnotes because hypoxia directly interacts with oxygen delivery, autonomic stress, and cardiovascular response.
Stop the session immediately and seek urgent care if you experience chest pain or pressure, fainting, severe shortness of breath, new neurological symptoms such as weakness, slurred speech, or visual changes, sustained palpitations, or a severe headache unlike your usual headaches. These are not “adaptation symptoms.”
More common warning signs include dizziness, headache, nausea, excessive air hunger, tingling, anxiety escalation, unusual fatigue, poor sleep, or a next-day resting heart rate rise. These do not automatically mean something dangerous happened, but they do mean the dose, timing, or method may be wrong for you.
Evidence and limits
The evidence on intermittent hypoxia is heterogeneous. It includes animal models, small human trials, athlete studies, device-based interventions, clinical rehabilitation research, and mechanistic physiology work. Those categories do not answer the same question. A supervised clinical protocol in a patient group does not prove that a consumer device improves performance in a healthy athlete.
The biggest limitation is protocol variability. Studies and clinics differ in oxygen depth, interval length, number of cycles, exercise intensity, recovery gas, program duration, and participant selection. That makes it difficult to name one standard protocol or promise a predictable outcome. Without external sources provided for this article, specific numerical claims about FiO2 ranges, altitude equivalents, VO2max changes, blood pressure effects, or disease outcomes should not be treated as established here.
The most defensible practical takeaway is that intermittent hypoxia may act as a stressor with potential adaptive effects in some contexts, but benefits are not guaranteed and harms are dose-dependent. The smarter standard is not “Does hypoxia work?” It is “For this person, with this baseline, using this device, at this dose, does the next week look better or worse?”
Conservative strategies to discuss with a professional
Choose the method by oversight, not novelty
The lowest-risk route for anyone with medical complexity is a supervised clinical setting where screening, monitoring, and stop rules are built in. Device-based normobaric hypoxia can be more controllable than improvised methods, but device quality and safety controls vary. Altitude rooms and tents create different exposure patterns and can affect sleep. Travel to altitude adds training, hydration, temperature, and recovery variables at the same time.
Breath-holding deserves a separate caution. It is not a safe substitute for device-based intermittent hypoxia, especially during exercise, in water, or when done competitively. If the goal is relaxation, breathwork that does not deliberately chase hypoxia is a different category.
Protocol example 1: hypoxia familiarization
This commonly used conservative structure is designed to assess tolerance with minimal complexity. It is an example to discuss with a qualified professional, not an individualized prescription.
- Goal: Assess tolerance with clear stop rules and low overall stress.
- Session structure: 20 to 30 minutes total, starting with 5 minutes of normoxic breathing, followed by 4 to 6 cycles of 2 to 3 minutes of hypoxia plus 2 to 3 minutes of normoxia, then 5 minutes of normoxic cool-down.
- Intensity: Mostly Zone 1 to low Zone 2. RPE 2 to 4 out of 10. If paired with light movement, effort should stay conversational.
- Weekly schedule: Minimal exposure is 1 session per week. A standard conservative structure is 2 non-consecutive sessions per week. A more advanced structure might add 1 optional low-stress session only when readiness markers are stable.
- Readiness gates: Do not progress if your 3 to 7 day HRV trend is meaningfully down versus baseline, morning resting heart rate is elevated for 2 to 3 days, sleep has been poor for 2 nights, or soreness and fatigue are significant. HRV is a decision-support tool, not an oracle.
Protocol example 2: IHT with low-impact aerobic work
This structure is for people who already tolerate aerobic training and want to combine hypoxic exposure with controlled movement. It should replace training stress, not simply add to it.
- Goal: Combine hypoxic stress with easy to moderate aerobic work without turning the session into maximal training.
- Session structure: 35 to 50 minutes total, with 10 minutes of easy normoxic warm-up, then 3 to 5 blocks of 4 minutes hypoxia plus 4 minutes normoxia while cycling, rowing, or walking briskly on an incline, followed by 10 minutes of easy normoxic cool-down.
- Intensity: Zone 2 during hypoxia blocks, avoiding sustained Zone 3. RPE 4 to 6 out of 10. Reduce pace or power during hypoxia to keep internal load controlled.
- Weekly schedule: Often used as 1 session per week in place of a Zone 2 session. Some programs use 1 to 2 sessions per week replacing, not adding to, intense work. More is not automatically better.
- Readiness gates: Proceed only when HRV trend is stable or improving, resting heart rate is within your personal normal range, sleep was good, and the session is not paired with a lower-body strength day.
- Stop rule: If hypoxia creates breathing distress, dizziness, chest discomfort, or escalating anxiety, end the block and return to normoxia.
If your current program already includes high-intensity work, be careful with stacking. A hard all about hiit workout plan session, all about tabata high intensity workout, sauna, fasting, poor sleep, and hypoxia can add up quickly even if each item looks reasonable alone.
Protocol example 3: 10 to 15 minute microdose
This structure is meant for busy professionals who want a low-cognitive-load exposure and are not chasing extremes.
- Goal: Build consistency and observe response without making hypoxia the centerpiece of the day.
- Session structure: 10 to 15 minutes total, starting with 3 minutes normoxia, followed by 3 to 4 cycles of 60 to 90 seconds mild hypoxia plus 90 seconds normoxia, then 2 minutes normoxia to finish.
- Intensity: Seated, Zone 1, RPE 2 to 3 out of 10.
- Weekly schedule: 1 session per week is a minimalist approach. 2 sessions per week is a common conservative structure. Breathwork-only relaxation on other days should not be treated as added hypoxia.
- Skip conditions: Skip if you have a headache, acute illness, poor sleep, elevated resting heart rate, unusual anxiety, or heavy fatigue.
Progress one variable at a time
If you progress, change only one variable: oxygen depth, interval length, cycle count, movement intensity, or weekly frequency. Changing several at once makes it hard to know what caused symptoms or performance changes. Deload weeks are not a sign the protocol failed. They are how stress-based training remains trainable.
For endurance athletes, intermittent hypoxia should not replace the fundamentals of sport-specific capacity. A swimmer thinking about vo2max swimming still needs water-specific mechanics and intervals. A runner coming back after a long race should prioritize recovery after marathon before adding another stressor.
How to track and interpret changes
Tracking should answer one question: did the exposure improve your training week or quietly degrade it? The useful signals are not just during-session oxygen data. The next morning often tells you more about whether the dose was appropriate.
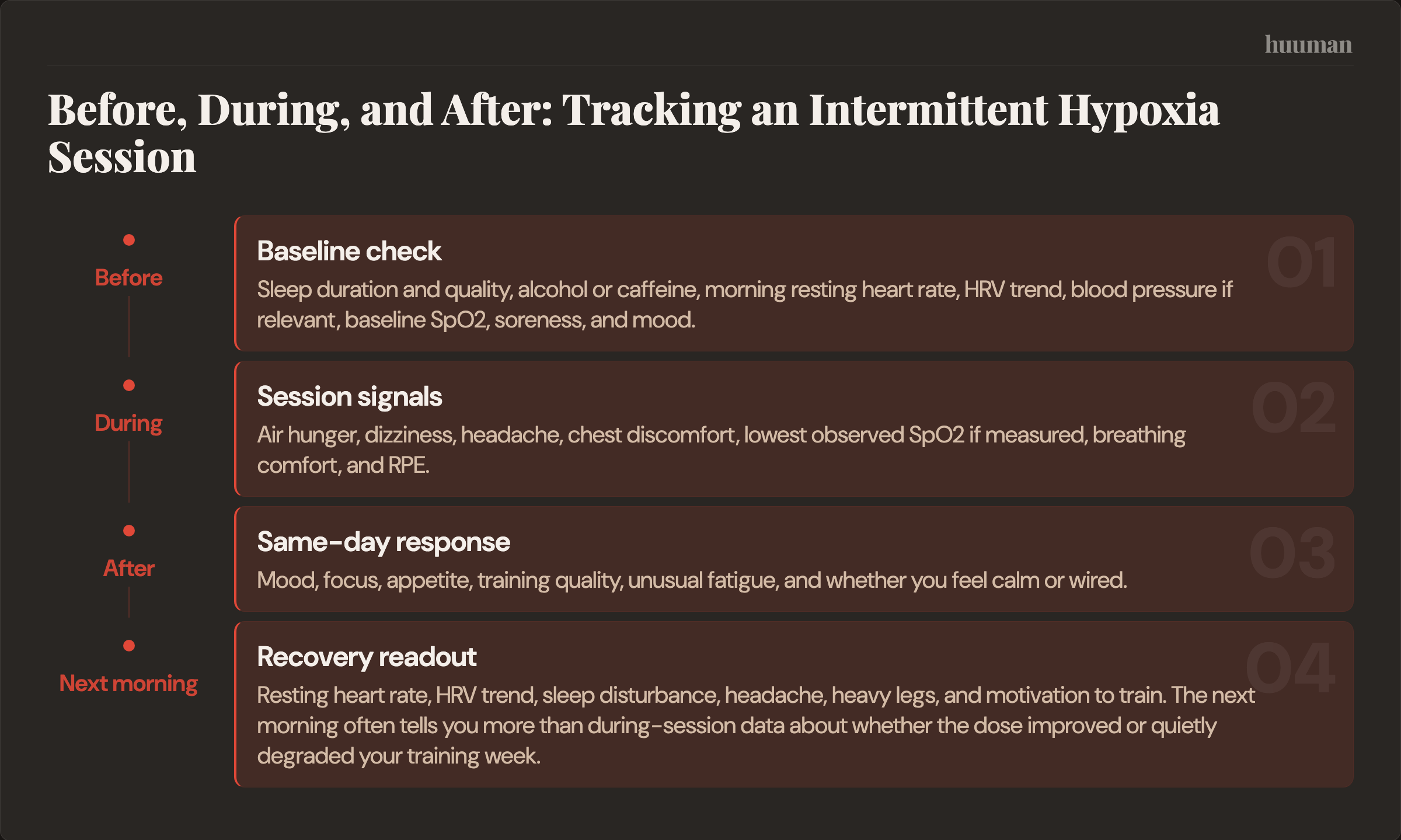
- Before the session: Sleep duration and quality, alcohol or caffeine, morning resting heart rate, HRV trend, blood pressure if relevant, baseline SpO2, soreness, and mood.
- During the session: Air hunger, dizziness, headache, chest discomfort, lowest observed SpO2 if measured, breathing comfort, and RPE.
- After the session: Mood, focus, appetite, training quality, unusual fatigue, and whether you feel calm or wired.
- Next morning: Resting heart rate, HRV trend, sleep disturbance, headache, heavy legs, and motivation to train.
A useful baseline is 7 to 14 days of normal tracking before adding intermittent hypoxia. Without baseline data, a low HRV day or elevated resting heart rate may be overinterpreted. With baseline data, you can identify whether the pattern changed after a session or whether it was already happening.
Filled example tracking log
- Date and session: Tuesday, 7:30 a.m., seated hypoxia familiarization, 4 cycles of 2 minutes hypoxia plus 3 minutes normoxia.
- Before: Sleep 7 hours 20 minutes, no alcohol, one coffee, morning RHR within normal range, HRV trend stable, baseline SpO2 normal for personal device readings, no soreness.
- During: RPE 3 out of 10, mild air hunger on cycles 3 and 4, no dizziness, no headache, no chest symptoms, lowest observed SpO2 recorded as a context marker rather than a target.
- After same day: Focus slightly better for 2 hours, appetite normal, easy walk felt normal, no need for extra stimulants.
- Next morning: Sleep undisturbed, RHR still normal, HRV trend unchanged, no headache, training readiness normal. Interpretation: repeat same dose before considering progression.
For structured training weeks, this matters more than a single session feeling novel. If you are already doing a compact program such as a one and done workout, adding hypoxia should not make the plan harder to recover from.
Rather than forcing a rigid schedule, your huuman Coach can adapt weekly strength, cardio, and recovery plans around your sleep, recovery, training load, goals, and available time.
Signal vs noise in intermittent hypoxia
- SpO2 is context, not a score. A lower number does not prove a better session; compare it with symptoms and next-day recovery before changing anything.
- Lower oxygen is not automatically better. If the only way to feel successful is to chase deeper hypoxia, reduce the dose and define success by repeatability.
- OSA-style hypoxia is not training. If you snore heavily, wake gasping, or feel unrefreshed despite enough sleep, prioritize sleep evaluation before experimenting.
- Worse sleep is a warning sign. If a session leaves you wired at night or seems to fragment sleep, consider moving it earlier, reducing the dose, or stopping the block.
- Heart rate can lag on short intervals. For brief hypoxic blocks, use RPE, breathing comfort, and pace or power restraint rather than waiting for heart rate to catch up.
- HRV is a decision-support tool, not an oracle. Use trends over several days and pair them with resting heart rate, mood, and training quality.
- Stimulant dependence means the stress budget is off. If you need extra caffeine to tolerate sessions or train afterward, reduce total load first.
- Novelty can masquerade as benefit. Feeling alert after a new stimulus is not the same as improved performance; look for stable sleep, normal readiness, and better training quality over weeks.
- Basics still win. National guidelines anchor the foundation in 150 minutes of weekly aerobic activity plus muscle-strengthening on 2 or more days. If that base, along with protein intake and sleep, is inconsistent, steady those before adding hypoxic complexity.
Common questions
What is intermittent hypoxia, and how is it different from altitude training?
Intermittent hypoxia alternates lower-oxygen exposure with normal-air recovery. Altitude training usually involves a broader environmental exposure, often affecting sleep, daily activity, hydration, and training. Intermittent protocols are more controlled, but their effects remain incompletely understood and should not be assumed to match the adaptations of living or training at altitude.
Is intermittent hypoxia the same thing as sleep apnea-related hypoxia?
No. Sleep apnea-related intermittent hypoxia is generally an uncontrolled risk exposure paired with disrupted sleep and repeated stress responses. Intentional intermittent hypoxia is structured, time-limited, and ideally monitored. Suspected OSA is a reason to seek evaluation, not a reason to start hypoxia training.
What are the potential benefits for endurance and metabolic health?
People look for improved tolerance to hard aerobic work, better breathing comfort, vascular effects, metabolic flexibility, and recovery-related changes. Evidence suggests possible effects in some contexts, but results depend heavily on protocol, baseline fitness, sleep, iron status, training load, and medical status. Treat benefits as possible, not promised.
Who should avoid intermittent hypoxia or get medical input first?
Get clinician input first if you have suspected or known OSA, uncontrolled hypertension, arrhythmias, heart or lung disease, pregnancy, prior stroke, seizure disorder, anemia or iron deficiency, severe panic susceptibility, or unexplained symptoms with exercise. Stop urgently for chest pressure, fainting, severe breathlessness, new neurological symptoms, sustained palpitations, or a severe unusual headache.
How often should a conservative protocol be done?
Common conservative examples use 1 to 2 weekly sessions at first, especially when hypoxia is added to an existing training plan. More frequent exposure should be treated as progression, not a default. If sleep, resting heart rate, HRV trend, mood, or training quality worsens, the dose is probably too aggressive.
What should I track during intermittent hypoxia?
Track baseline sleep, resting heart rate, HRV trend, caffeine or alcohol, blood pressure if relevant, baseline SpO2, symptoms during the session, RPE, lowest observed SpO2 if measured, same-day mood and appetite, and next-morning readiness. The pattern matters more than any single metric.
Is IHHT better than standard intermittent hypoxia?
IHHT alternates hypoxia with hyperoxia, while standard intermittent hypoxia usually returns to normoxia during recovery segments. The theoretical appeal is different recovery gas exposure, but protocols vary and results are inconsistent, so the evidence is not strong enough to declare IHHT universally superior. Safety controls and individual response matter more than the label.
If you are unsure whether the pattern is helping or just adding stress, your huuman Coach can interpret trends before you change the dose and help you decide whether to hold, reduce.
Intermittent hypoxia is best viewed as an optional advanced stressor. It should earn its place by improving the training week, not by sounding more sophisticated than ordinary aerobic work, strength training, and sleep. The safest path is conservative exposure, clear stop rules, and honest tracking.
More health topics to explore
- Heart & Cardio – Overview
- VO2max: what it means, what counts as a good value, and how to interpret it properly
- Understanding HRV: Charts, Normal Ranges, and What “Good” Really Means
- Strokes Per Minute: What’s a Good Rate for Rowing?
References
- Frontiers — Frontiers | Intermittent Hypoxic Training as an Effective Tool for...
- Villa JG et al. — Does intermittent hypoxia increase erythropoiesis in professional cyclists... (2005)
- Kasperska A & Zembron-Lacny A — The effect of intermittent hypoxic exposure on erythropoietic response and... (2020)
- Gonzalez-Rothi EJ et al. — Intermittent hypoxia and neurorehabilitation (2015)
- WHO — Who Ps Pulse Oxymetry Training Manual En
- Powell et al. — HIF-1 and ventilatory acclimatization to chronic hypoxia. (2008)
- Vijayan et al. — Morbidities associated with obstructive sleep apnea. (2012)
- Saunders et al. — Comparison of live high: train low altitude and intermittent hypoxic exposure. (2013)
- Suleiman et al. — Neuroanatomical and pharmaco-physiological effects of hypoxia and esketamine on breathing, the sympathetic nerve system, and cortical function. (2025)
- Glazachev OS et al. — Safety and Efficacy of Intermittent Hypoxia Conditioning as a New... (2021)
- Rusko HK et al. — Altitude and endurance training (2004)
- Destors M et al. — [Pathophysiology of obstructive sleep apnea syndrome and its cardiometabolic... (2017)
- CDC — Physical Activity Guidelines for Adults
- Cleveland Clinic — Hypoxemia
About this article · Written by the huuman Team. Our content is based on peer-reviewed research and clinical guidelines. We follow editorial standards grounded in scientific evidence.
This article is for educational purposes only and does not constitute medical advice. Health and training decisions should be discussed with qualified professionals.