

VO2max measures how much oxygen your body can use during peak exercise. It reflects the combined efficiency of your heart, lungs, blood vessels, and muscles working together. As a single number, it captures more about your body's overall function than almost any other metric available.
In 2018, a study of 122,007 patients at the Cleveland Clinic found that low cardiorespiratory fitness was associated with higher mortality risk than smoking, diabetes, or coronary artery disease. That finding landed hard in longevity research, and for good reason: it reframes fitness from a lifestyle choice into a clinical risk factor.
But the number alone isn't useful unless you know what to do with it. This article covers the evidence, what the ranges mean for different people, how to measure and track it, and exactly how to improve it.
What VO2max actually measures
VO2max is your maximal oxygen uptake, expressed in milliliters of oxygen per kilogram of body weight per minute (mL/kg/min). During a graded exercise test, you work harder and harder until your body physically cannot consume more oxygen. That ceiling is your VO2max. It reflects four systems working in sequence: your lungs absorb oxygen, your heart pumps oxygenated blood, your blood vessels deliver it to working muscles, and your mitochondria use it to produce energy. A limitation anywhere in that chain lowers the number. This is why VO2max is considered a systems-level biomarker. It doesn't just measure your heart. It measures how well your cardiovascular, pulmonary, metabolic, and muscular systems integrate under stress.
The evidence: what the large studies found
Mandsager et al. (2018) retrospectively analyzed 122,007 patients who underwent exercise treadmill testing at the Cleveland Clinic between 1991 and 2014, with a median follow-up of 8.4 years. The key findings:
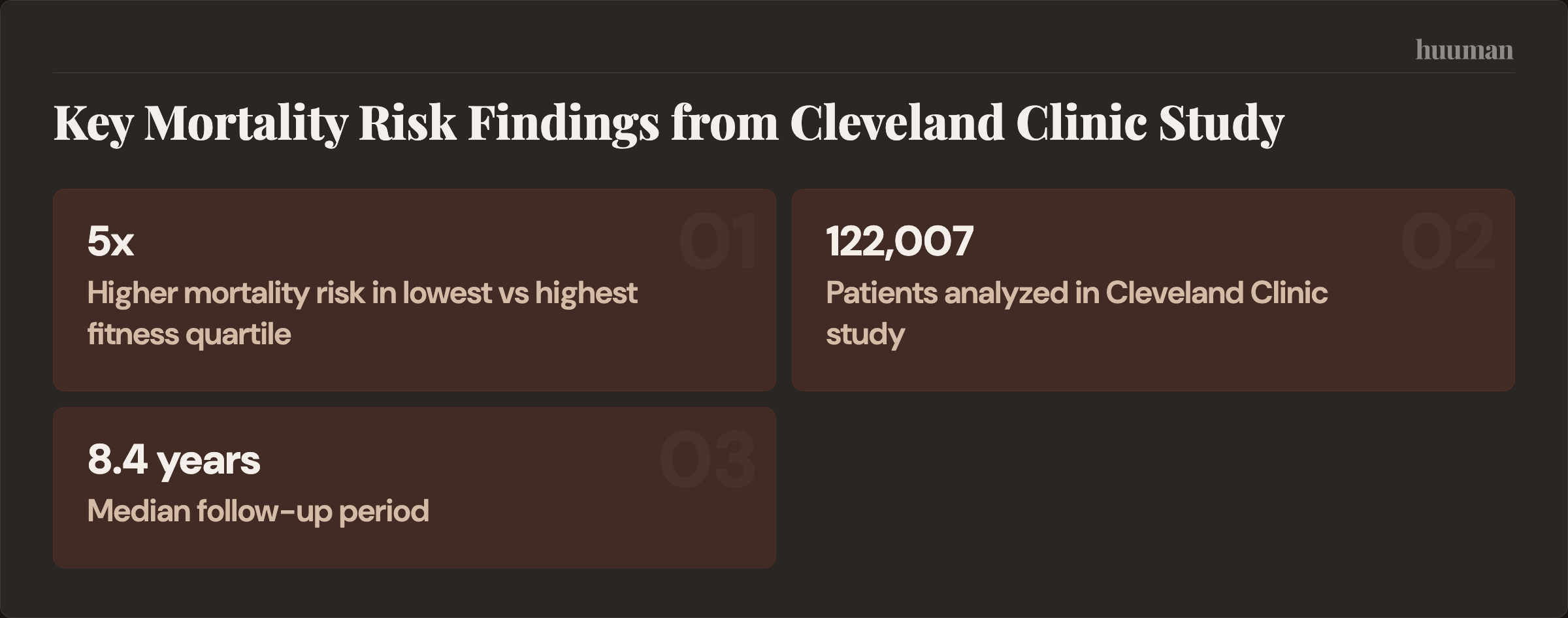
- Patients in the lowest fitness quartile had nearly 5 times the mortality risk of those in the highest quartile.
- Low cardiorespiratory fitness was associated with higher mortality risk than smoking, diabetes, or coronary artery disease.
- There was no upper limit of benefit. The fittest group had the best outcomes, with no plateau.
- The steepest benefit curve was at the bottom: moving from "low" to "below average" fitness produced larger risk reductions than moving from "above average" to "elite."
That last point is the most practically important. If you're currently inactive, the biggest longevity return on investment isn't training for a marathon. It's building a basic aerobic foundation.
Context and limitations
This was a retrospective observational study at a single institution. The patients were referred for exercise testing, which may introduce selection bias. The study demonstrates a strong association, not a proven causal pathway. However, the effect size is large, the dose-response relationship is consistent, and the findings align with decades of prior research from the Cooper Center Longitudinal Study and other cohorts. The responsible interpretation: improving cardiovascular fitness is very likely to reduce your mortality risk, and the magnitude of that benefit is among the largest in preventive medicine. But individual results depend on genetics, baseline health, adherence, and other factors.
What the ranges mean
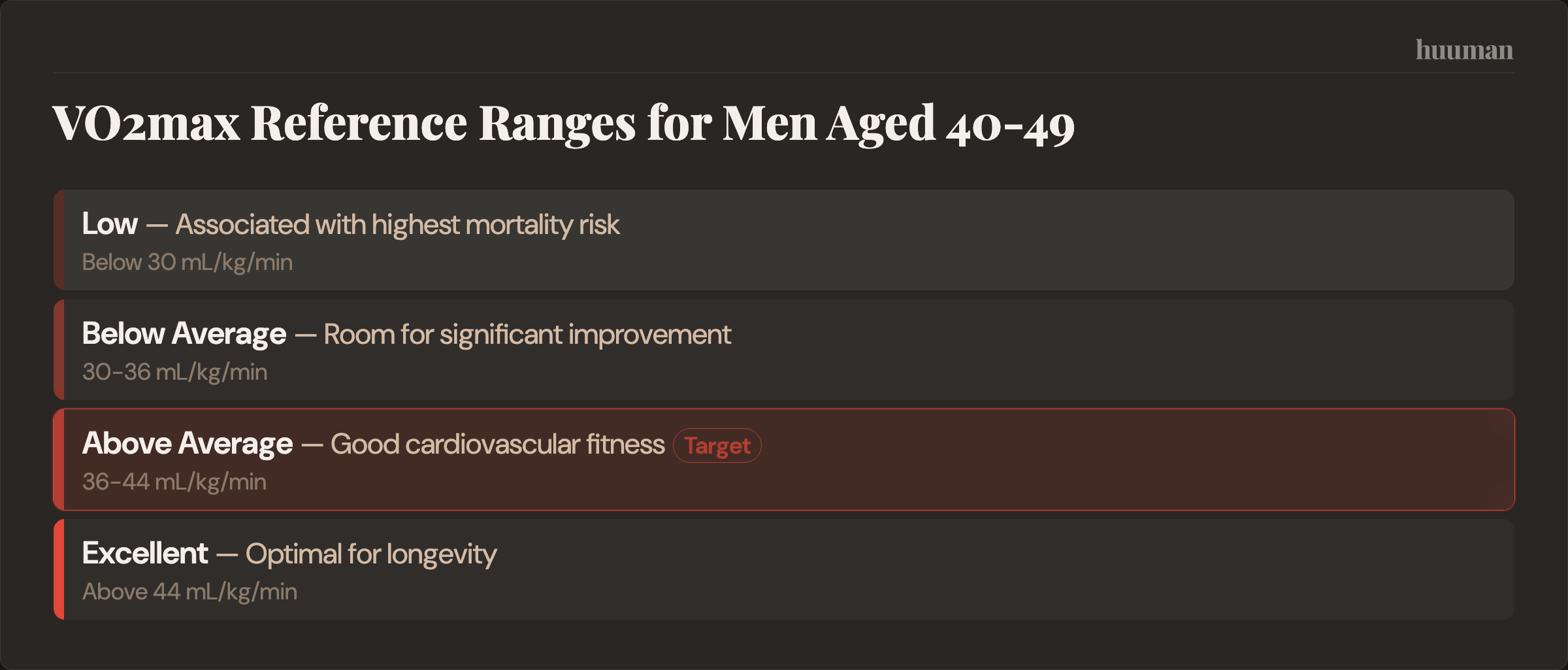
Raw VO2max values are most useful when compared to age- and sex-matched norms. Here are general reference ranges: Men aged 40–49: Below 30 mL/kg/min = low. 30–36 = below average. 36–44 = above average. Above 44 = excellent. Women aged 40–49: Below 22 mL/kg/min = low. 22–28 = below average. 28–36 = above average. Above 36 = excellent. These shift downward with age and upward with training history. The clinical cutoff that matters most, based on the Mandsager data, is the bottom 25th percentile for your age and sex. Being in that bottom quartile carries the steepest risk. Getting out of it provides the largest benefit.
When the number is misleading
VO2max expressed per kilogram of body weight can understate fitness in people with higher body mass. A person at 110 kg with strong cardiovascular function may show a lower relative VO2max than a lighter person with weaker absolute capacity. Absolute VO2max (L/min) can provide additional context. Wearable estimates can also be misleading during periods of illness, medication changes (beta-blockers suppress heart rate), altitude acclimatization, or detraining. A sudden drop in your watch's VO2max estimate after starting a blood pressure medication isn't a fitness decline. It's a measurement artifact. If you're making clinical decisions based on VO2max, a lab test is worth the investment. For trend tracking, wearable estimates work well as long as you understand their limitations.
Why it reflects more than heart health
VO2max predicts outcomes across disease categories because it reflects multi-system function:
- Cardiovascular: Cardiac output, vascular health, blood pressure regulation
- Metabolic: Mitochondrial density, insulin sensitivity, fat oxidation capacity
- Muscular: Oxygen extraction at tissue level, capillary density
- Neurological: Higher VO2max is associated with greater brain volume and better cognitive function, with reduced risk of dementia
When cardiovascular fitness improves, it doesn't just strengthen the heart. It shifts your entire physiology: better metabolic regulation, improved sleep quality and recovery, enhanced cognitive function, and greater resilience to stress. This is why it connects to all five areas of health, not just Heart. You can sync your Apple Health data with the huuman app to track cardiovascular trends alongside sleep efficiency, resting heart rate, and recovery patterns across all five domains.
The age-related decline and how to fight it
VO2max declines approximately 10% per decade after age 30 in sedentary individuals. By 70, an inactive person may have lost half their peak aerobic capacity. This maps directly to functional ability: the capacity to climb stairs, carry groceries, travel independently, recover from illness. The rate of decline is highly modifiable. Regularly active individuals lose roughly 5% per decade instead of 10%. Masters athletes in their 70s and 80s maintain VO2max values comparable to inactive 40-year-olds. The practical implication: if you want to hike, travel, and live independently at 80, the cardiovascular fitness you build and maintain now directly determines what you'll be able to do. This is the core of primespan thinking: maintaining the physical capability that makes long life worth living. It is also at the heart of why huuman was built.
How to measure it
Lab testing (most accurate)
A graded exercise test (GXT) with a metabolic cart directly measures oxygen consumption as you exercise to exhaustion. Cost ranges from $150–$400 at sports medicine clinics and university labs. Worth doing once to establish a precise baseline, and periodically (annually or every 2 years) to validate wearable trends. Consider a lab test if: you're starting a serious training program, you have cardiovascular risk factors, your wearable trend doesn't match how you feel, or you want a precise baseline for goal-setting.
Wearable estimates (good for trends)
Apple Watch, Garmin, COROS, and Whoop estimate VO2max from heart rate data during outdoor exercise. These estimates may be 5–15% off from lab values, but they're useful for tracking direction over weeks and months. Wearable estimates are sufficient if: you're primarily tracking whether your fitness is improving, stable, or declining. The trend matters more than the absolute number for most people.
Field tests (no equipment needed)
The Cooper 12-minute run test (distance covered maps to estimated VO2max) and the Rockport 1-mile walk test are validated assessments you can do anywhere. Useful for establishing a rough baseline if you don't have a wearable.
How to improve it
VO2max responds reliably to training. The research supports a two-component approach: a large base of moderate-intensity aerobic work, plus a smaller dose of high-intensity training.
A meta-analysis of training studies found that higher intensity training produces greater VO2max improvements in young adults, supporting the value of including high-intensity work.
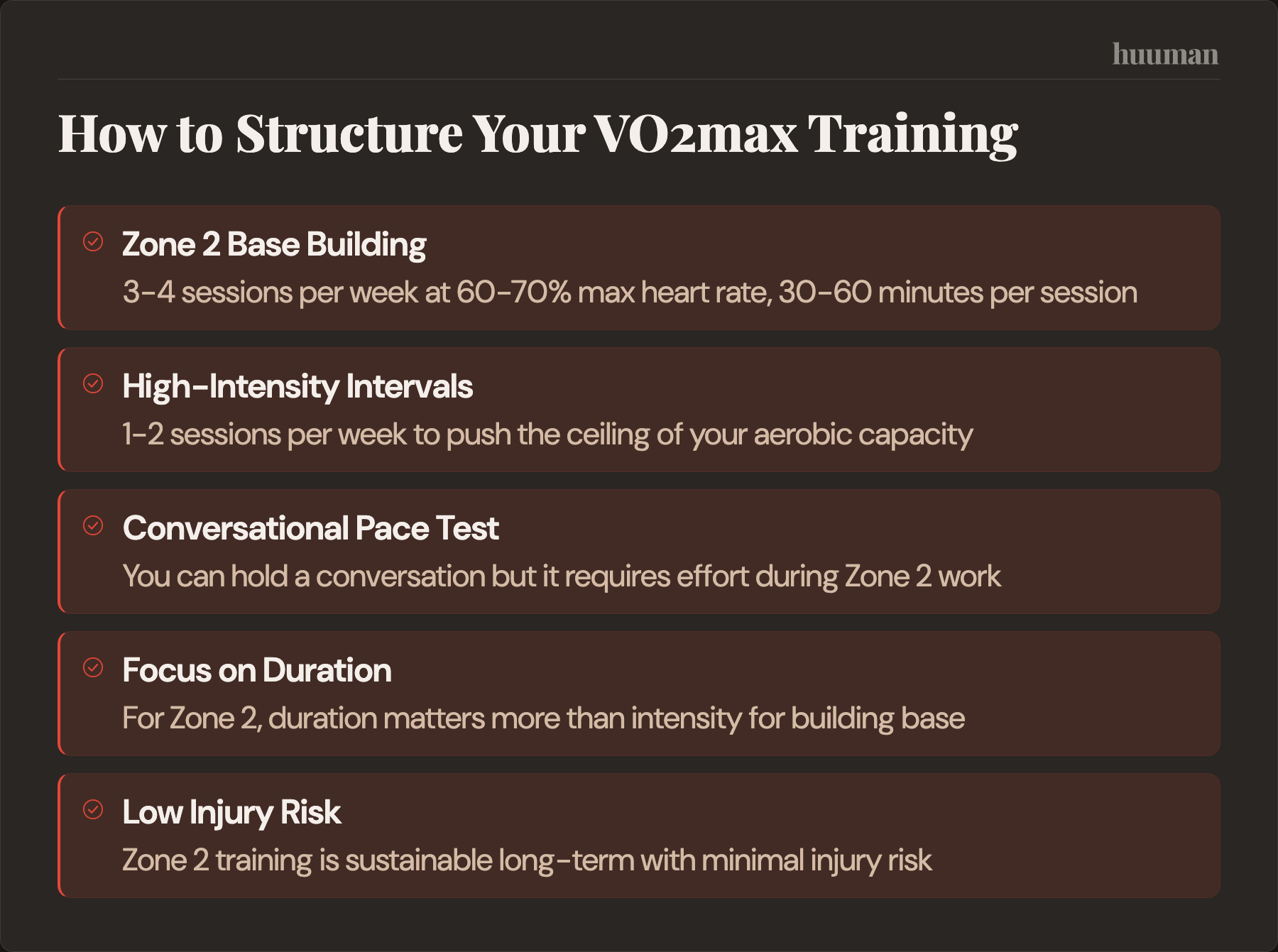
Zone 2: the aerobic foundation (3–4 sessions/week)
Zone 2 is steady-state exercise at an intensity where you can hold a conversation but it requires effort, typically 60–70% of maximum heart rate. At this intensity, your body primarily uses fat oxidation and mitochondrial respiration.
- Increases mitochondrial density and function
- Improves fat oxidation capacity
- Enhances capillary density in working muscles
- Builds cardiac stroke volume
- Low injury risk, sustainable long-term
Duration matters more than intensity. Aim for 30–60 minutes per session. Walking, cycling, swimming, rowing: the modality matters less than consistently hitting the right intensity.
High-intensity intervals: the ceiling raiser (1–2 sessions/week)
While Zone 2 builds the base, high-intensity interval training pushes the ceiling. Intervals at 85–95% of max heart rate specifically challenge and improve VO2max. The most studied protocol: the 4x4 Norwegian method. Four rounds of 4 minutes at 85–95% max HR, separated by 3 minutes of active recovery. Wisløff et al. (2007) in Circulation showed this approach improved VO2max by 46% in heart failure patients over 12 weeks. Other effective formats:
- 30/30s: 30 seconds hard, 30 seconds easy, 15–20 minutes. Accessible for beginners.
- Tempo runs: 20–40 minutes at "comfortably hard" pace. Improves lactate clearance.
One to two HIIT sessions per week is optimal for most people. More increases injury risk, impairs recovery, and disrupts sleep. The 80/20 rule applies: roughly 80% of training volume at Zone 2, 20% at high intensity.
Sample weekly structure
- Monday: 45 min Zone 2 (cycling or brisk walking)
- Tuesday: Strength training
- Wednesday: 4x4 intervals (running, rowing, or cycling)
- Thursday: 45 min Zone 2
- Friday: Strength training
- Saturday: 60+ min Zone 2 (hike, long walk, easy bike)
- Sunday: Rest or easy movement
What to do if your VO2max is declining
A downward trend over 3+ months warrants attention. Here's how to think through it: Check measurement quality first. Did you change devices, start a new medication, move to a different altitude, or switch from outdoor to treadmill exercise? Wearable estimates are sensitive to these changes. Compare against a field test or lab test before assuming real decline. Review your training structure. The most common cause of stagnation or decline is too much moderate-intensity work and not enough true Zone 2 or true high-intensity training. If every run is "kind of hard," you're likely training in the dead zone where neither base nor ceiling improves. Check recovery factors. Chronic sleep debt, sustained high stress, overtraining, or poor nutrition can all suppress cardiovascular adaptation. If training volume is adequate but VO2max is still falling, the problem may be recovery, not stimulus. Consider a medical evaluation. In people over 50, a persistent decline despite adequate training and recovery may warrant a cardiology workup. New exercise intolerance, unusual breathlessness, or chest discomfort during exertion should always be evaluated by a physician.
Where most people go wrong
Too much intensity, not enough base. The most common mistake is spending too much time in the "moderate" zone: too hard to build aerobic capacity, too easy to push VO2max higher. Three easy conversations-pace sessions per week do more for most people than five "medium-hard" ones. Inconsistency. Three months of dedicated training followed by six months off doesn't build lasting fitness. VO2max responds to year-round consistency. Even two sessions per week during busy periods preserves most gains. Ignoring the trend. A single measurement is a snapshot. What matters is the trajectory over months and years. Track it the same way you'd track body weight or blood markers: look for direction, not daily noise.
Common questions
What is a good VO2max for my age?
It depends on age and sex. For men aged 40–49, above 36 mL/kg/min is above average; above 44 is excellent. For women, above 28 is above average; above 36 is excellent. The most clinically meaningful threshold is avoiding the bottom 25th percentile for your age group, where mortality risk rises steeply.
Can you improve VO2max after 50?
Yes. Studies consistently show that previously sedentary adults in their 50s, 60s, and 70s can improve VO2max by 15–25% with structured training. The physiological response to training doesn't disappear with age. It requires consistency and appropriate progression.
A randomized controlled trial found that adults with chronic kidney disease improved their cardiorespiratory fitness with long-term exercise training.
How long does it take to see improvement?
Most people see measurable changes within 4–8 weeks. Significant gains (10–20%) typically require 3–6 months. The steepest improvements come early and from lower baselines.
Is VO2max or resting heart rate more important?
VO2max is far more strongly associated with mortality and overall health. Resting heart rate is a useful daily signal (lower is generally better, trends matter), but it doesn't capture multi-system function the way VO2max does.
Should I get a lab test or just use my watch?
For most people, wearable trend tracking is sufficient. Consider a lab test if you're establishing a baseline for serious training, have cardiovascular risk factors, or notice a persistent discrepancy between how you feel and what your device reports. Your VO2max is one of the most actionable health metrics you can track because it reflects your entire physiological system under stress. Your huuman Coach builds personalized weekly training plans that balance Zone 2 and interval work based on your current fitness level, recovery signals, and capacity for progression.
More health topics to explore
- Heart & Cardio – Overview
- HIIT for Cardio: How to Do It Safely, Effectively, and Without Burning Out
- Zone 2 Heart Rate Calculator: How to Verify Your True Zone 2
- How to Improve VO2max: Interval and Zone 2 Training Plan with Tracking
References
- Ross et al. — Importance of Assessing Cardiorespiratory Fitness (AHA Scientific Statement, 2016)
- Blair et al. — Physical Fitness and All-Cause Mortality (Cooper Center Longitudinal Study, 1989)
- Tarumi et al. — Aerobic Exercise Training and Neurocognitive Function in Older Adults (2022)
- Hawkins & Wiswell — Rate and Mechanism of Maximal Oxygen Consumption Decline with Aging (2003)
- Milanović et al. — HIT vs Continuous Training for VO2max (2015)
- Scribbans TD et al. 2016 — The Effect of Training Intensity on VO(2)max in Young Healthy Adults: A Meta-Regression and Meta-Analysis.
- Weiner DE et al. 2023 — Effect of Long-term Exercise Training on Physical Performance and Cardiorespiratory Function in Adults With CKD
About this article · Written by the huuman Team. Our content is based on peer-reviewed research and clinical guidelines. We follow editorial standards grounded in scientific evidence.
This article is for educational purposes only and does not constitute medical advice. Health and training decisions should be discussed with qualified professionals.

