You crossed the line. Now comes the part most people underestimate: what happens after marathon day determines how quickly you feel like yourself again and how safely you get back to running.
That "wrecked but wired" mix is normal. A marathon stresses multiple systems at once: muscle fibers, tendons and joints, fuel stores, hydration balance, your nervous system, and even your mood. Recovery is not just about sore legs.
Key takeaways
1. 0–24 hours: eat a carb-forward meal with protein, sip fluids with electrolytes, keep moving with easy walking, get warm and dry, protect sleep.
2. Days 2–7: shift to low-intensity activity like walking, cycling, or swimming. Keep effort easy. Reintroduce short jogs only if soreness is low and improving.
3. Weeks 2–4: rebuild frequency before intensity. Start with short easy runs, then extend duration. Add strides only when legs feel responsive.
This guide gives you a clear, time-based plan for after marathon recovery, plus a decision system for when to run again that blends how you feel with simple wearable signals. The goal is not to rush back, but to return with fewer setbacks.
Where this fits in your overall training
Think of the weeks after a marathon as a built-in deload. Many training cycles plan stress carefully, then neglect recovery when it matters most. Post-race weeks are where you consolidate adaptations and reduce injury risk.
This is also where basics carry the most leverage: sleep, energy intake, hydration, and low-intensity movement. If you want more context on how these pieces interact, the Sleep & Recovery overview and a deeper look at running recovery in depth help frame the bigger picture.
Quick answer
After a marathon, prioritize three things: restore fluids and carbs, reduce soreness with gentle movement, and give your nervous system real rest.
- 0–24 hours: eat a carb-forward meal with protein, sip fluids with electrolytes, keep moving with easy walking, get warm and dry, protect sleep.
- Days 2–7: shift to low-intensity activity like walking, cycling, or swimming. Keep effort easy. Reintroduce short jogs only if soreness is low and improving.
- Weeks 2–4: rebuild frequency before intensity. Start with short easy runs, then extend duration. Add strides only when legs feel responsive.
- Readiness checks: resting heart rate back near baseline, HRV trend stabilizing, sleep normalized, soreness low, gait feels normal.
- What to avoid: hard workouts too early, aggressive stretching into pain, "testing fitness," and overdrinking plain water.
- Get medical help if: chest pain, shortness of breath at rest, fainting, confusion, one-sided calf swelling, fever, or dark urine.
Instead of guessing when you're ready, track your sleep efficiency and wake times through the huuman app to see when your nervous system has actually recovered from race day stress.
What your body is recovering from
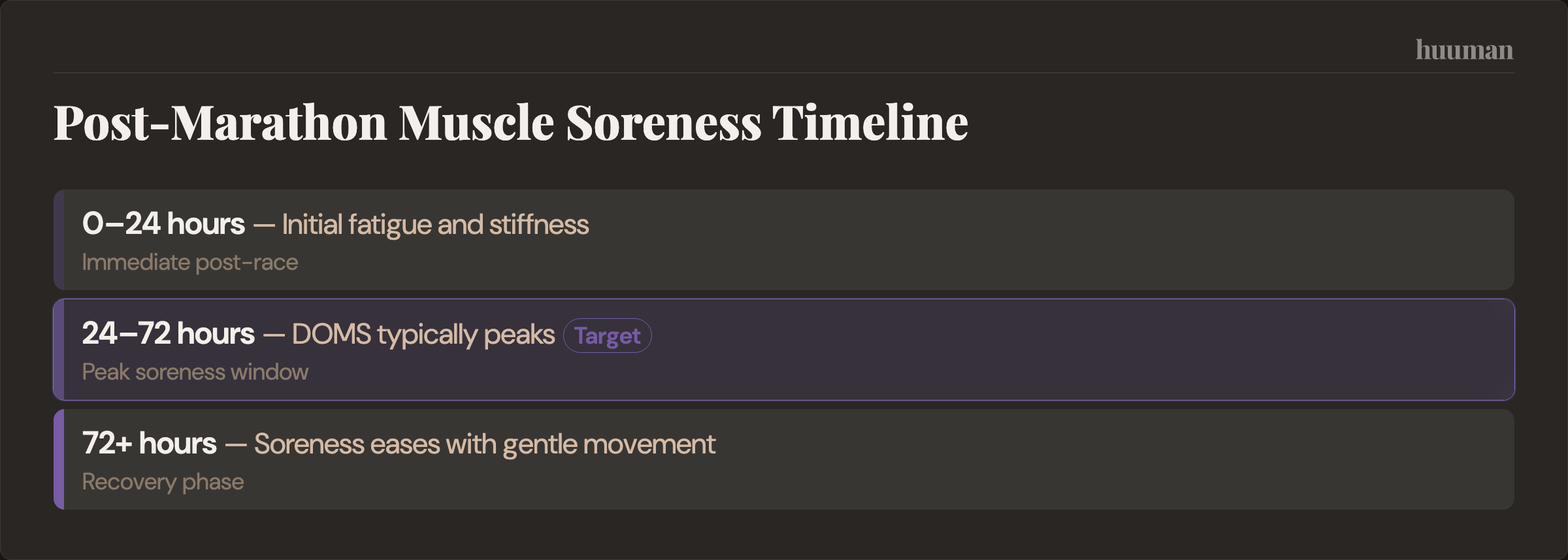
Muscle damage and DOMS. Microscopic damage accumulates over 42.2 km, especially with downhills and eccentric muscular contractions. Delayed onset muscle soreness typically peaks 24–72 hours after the race, then eases if you keep moving gently. This is different from focal pain that sharpens with load.
Biomarkers of fatigue. Lab markers like creatine kinase can rise after a marathon and stay elevated for days. You do not need to test them. The point is that internal recovery often lags how you feel on a single day, which is why a cautious ramp matters.
Glycogen depletion. You finish with low muscle glycogen. Refueling restores energy availability and supports repair. Appetite may be blunted immediately, then rebound.
Hydration and sodium balance. You lose fluid and sodium through sweat. Rehydrating too slowly prolongs fatigue. Overcorrecting with only water can dilute sodium in the blood, which is risky. Balance matters.
Soft tissue and joints. Tendons, plantar fascia, and joint surfaces absorb repetitive load. They may feel fine right away and complain later. Treat them as the pacing factor for your return.
Nervous system and mood. High effort events can disrupt sleep and leave you flat or irritable for a few days. A mild "post-race blues" dip is common and usually passes.
The recovery timeline that matters
This is not a rigid schedule. It is a way to match actions to what your body is likely dealing with at each stage of recovery after marathon.

RESET Recovery Timeline (screenshot-friendly)
- Window: 0–6 hours - Main goals: Rehydrate, refuel, stabilize - What helps: Easy walking, change into dry clothes, carb-forward meal with protein, fluids with electrolytes - What to avoid: Long static stretching into pain, large alcohol intake, lying down for hours
- Window: 6–24 hours - Main goals: Start repair, protect sleep - What helps: Regular meals, light movement, short gentle mobility, early night - What to avoid: "Testing" pace, heavy strength work
- Window: Days 2–7 - Main goals: Reduce DOMS, restore normal gait - What helps: Walking, cycling, swimming, short jogs only if pain-free, light mobility - What to avoid: Workouts, hill sprints, long runs
- Window: Weeks 2–4 - Main goals: Return-to-run ramp - What helps: Short easy runs first, then duration, optional strides late - What to avoid: Stacking intensity and volume in the same week
- Window: Weeks 4–6+ - Main goals: Rebuild performance - What helps: Gradual reintroduction of workouts and a long run when fully ready - What to avoid: Jumping straight back to peak weeks
A common coaching approach is to allow a buffer of one to two weeks before structured running or workouts return, with variability based on how hard you raced and your training history. Treat that as a starting point, not a rule.
When can I run again? A simple decision system
Separate two questions: can you jog versus should you train. Many runners can jog before they should resume training.

Return-to-Run Checklist (save this)
- Gait feels normal on flat ground and stairs
- Soreness is ≤ 3/10 and improves during warm-up
- No focal pain at Achilles, knee, hip, or plantar fascia
- Resting heart rate is back near your baseline for several mornings
- HRV trend is stable or improving over a few days (use as guidance, not a verdict)
- Sleep duration and quality feel normal
- Mood and motivation are back to typical
If your watch says "ready" but your calf or foot disagrees, default to the tissue. Start with 20–30 minutes easy, add frequency first, then duration. Leave workouts for later.
Protocol cards you can follow
0–24 Hours After Marathon
- 10–20 minutes very easy walking when safe
- Shower, warm, dry clothes
- First substantial meal: carb-forward with protein, include salty foods if you sweat heavily
- 5–10 minutes gentle mobility to comfort
- Stop if dizziness, worsening nausea, confusion, chest symptoms, or faintness
Days 2–7: Active recovery microcycle
- 2–4 easy sessions (walk, bike, or swim), mostly zone 1 to low zone 2
- Optional short jogs only if readiness gates are met
- Finish sessions feeling better than you started
Weeks 2–4: Return-to-run ramp
- Reintroduce running frequency first, then duration
- Keep effort easy, cap intensity
- Add short relaxed strides late in week 3–4 if legs feel springy
Strategies that actually move recovery forward
Hydration and electrolytes
Replace losses gradually with fluids that include sodium. Pale yellow urine and normal thirst are simple guides. Headaches, dizziness, and persistent fatigue can signal you undershot. Bloating, clear urine, and a "waterlogged" feeling can signal you overdid plain water.
Food and refueling
Prioritize total energy, carbohydrate to restore glycogen, and protein to support repair. In the first day or two, simple meals you tolerate well beat perfection. Spread intake across the day. Sports nutrition guidelines consistently emphasize timely carbohydrate plus protein after prolonged endurance work, but exact gram targets vary by body size and context, so keep it practical rather than numeric.
Movement: what helps vs what flares you
Easy walking is the default. Cycling and swimming add blood flow without impact. Mobility should be to comfort, not aggressive stretching into pain. If movement reduces stiffness and improves how you feel during and after, you are in the right zone.
Soreness tools and trade-offs
- Modality: Massage / foam rolling - When to use: Days 1–7, light to moderate pressure - Expected benefit: May reduce perceived soreness - Drawbacks / limits: Overdoing pressure can irritate tissue
- Modality: Compression garments - When to use: Travel or long standing periods - Expected benefit: Improved subjective perceptions of recovery - Drawbacks / limits: No significant improvement in muscular strength or markers of muscle damage
- Modality: Cold water immersion / contrast - When to use: First 24–72 hours if very sore - Expected benefit: Can reduce soreness sensation - Drawbacks / limits: may blunt some training adaptations; acceptable trade-off right after a race
- Modality: Heat / sauna - When to use: After initial swelling subsides - Expected benefit: Relaxation, comfort - Drawbacks / limits: Dehydration risk if overused
- Modality: NSAIDs - When to use: Only with professional guidance - Expected benefit: Pain relief - Drawbacks / limits: Potential kidney and GI risks, especially after endurance events
Sleep and nervous system
The first two nights have outsized impact. Prioritize a wind-down routine, limit late caffeine, and keep evenings low-key. If you struggle to settle, simple inputs like light exposure in the morning and relaxing audio can help. If relevant, explore options like sleep music to support a downshift.
Mind: the post-race dip
A drop in mood or motivation is common once the goal is over. Keep structure light: short walks, sunlight, social contact, and one or two small daily anchors. It usually resolves as sleep and energy normalize.
Evidence and limits
There is solid support for the basics: adequate sleep, sufficient energy intake with carbohydrates and protein, and low-intensity active recovery. These consistently align with better perceived recovery and function.
For modalities like compression, massage, and cold exposure, evidence is mixed. They can improve how you feel in the short term, which can be useful right after a race, but they are not magic. Avoid claims that any of them "flush toxins."
After a marathon, the immune system can be transiently perturbed, with some people noticing sore throat or fatigue. This is not universal and not deterministic. Practical takeaway: favor sleep, energy, and hygiene in the first days.
Recovery timelines vary. Coaching guidance often places a conservative buffer before resuming structured training, but individual context matters: how hard you raced, heat, course profile, fueling, and your training age influence recovery Polar.
Minimal effective dose (for busy weeks)
- Day 0–1: 20–40 minutes total easy walking split into short bouts, one carb-forward meal with protein, early night
- Days 2–7: 2–3 easy cardio sessions (20–45 minutes) and two brief mobility sessions
- Week 2 start: try two short easy runs only if readiness gates are met
If you also lift, treat this as a deload phase. Keep loads light and volumes low. If you need an example structure, a deload week example or a deload protocol in depth shows how to reduce stress without losing rhythm. Strength work for runners later can connect to a muscle building protocol once you are fully recovered, with considerations if you are building muscle in old age.
RED FLAGS: when to seek medical care
Chest pain or pressure, shortness of breath at rest, fainting, confusion, one-sided calf swelling or pain, fever, dark cola-colored urine, or inability to keep fluids down. These are not normal recovery signs.
How to track and interpret changes
Create a simple morning log: rate muscle soreness (0-10), record resting heart rate, note sleep quality, and assess walking comfort. Same time daily, before caffeine.
Recovery shows through patterns: resting heart rate drifting back toward baseline, soreness scores trending down day over day, and walking feeling smooth again. Watch for trends, not single data points.
Let these metrics guide your return. Your huuman Coach can build weekly plans that adapt your running progression based on how your recovery signals actually trend.
Signal vs noise after marathon recovery
- DOMS equals progress. Not exactly. It reflects muscle damage, not readiness. Next step: wait until soreness is low and improving before adding running.
- If you can jog, you can train. Early jogs are not green lights for workouts. Next step: keep week 2 runs easy and short.
- Stretch it out hard. Aggressive stretching can irritate tissue. Next step: keep mobility within comfort.
- More water is always better. Overdrinking plain water can be risky. Next step: include electrolytes and drink to thirst.
- HRV is the truth. Useful, not perfect. Travel, alcohol, and poor sleep affect it. Next step: combine HRV with soreness, sleep, and gait.
- Cold plunges fix everything. They can reduce soreness but are not required. Next step: use them for comfort, not as a cure.
- No pain the next day means you are fine. Tendons often lag. Next step: look at 24–48h responses before progressing.
- Social pressure to bounce back. Pushing early increases risk. Next step: follow your checklist, not your feed.
- "Detox" products help recovery. Not supported physiologically. Next step: prioritize sleep, food, fluids, and easy movement.
Common questions
How long does it take to recover after a marathon?
Many runners feel broadly normal within a couple of weeks, but full recovery can take longer depending on how hard you raced and your training background. Coaching guidance commonly uses a short buffer before structured training returns, with variability across individuals Hal Higdon.
When can I run again after a marathon?
When your checklist is green: low and improving soreness, normal gait, sleep back to baseline, and stable resting HR or HRV trend. Start with short easy runs in week 2 for many runners, but let your signals decide.
Is it normal to feel sick or get a sore throat after a marathon?
Some people notice mild immune symptoms or fatigue in the days after prolonged endurance events. It is usually transient. Prioritize sleep, food, and hygiene. Seek care if symptoms are severe or persistent.
Why are my legs still heavy a week later?
Lingering muscle damage, incomplete glycogen restoration, and nervous system fatigue may contribute. If heaviness is paired with focal pain or worsens when you run, step back and use cross-training for a few days.
Should I stretch or foam roll right after a marathon?
Light, comfortable mobility can feel good. Avoid deep stretching into pain immediately after the race. Foam rolling is fine if pressure is moderate and does not aggravate tissue.
Do ice baths, compression, or massage actually help?
They may reduce perceived soreness for some people, which can make the first days more comfortable. Evidence for faster recovery is mixed. Use them as tools, not requirements.
What should I eat and drink after a marathon?
A carb-forward meal with protein, plus fluids with electrolytes, is a practical starting point. Continue regular meals over the next days to restore energy availability and support repair.
More health topics to explore
- Sleep & Recovery – Overview
- Running Recovery: A Practical, Evidence-Aware Playbook for Runners
- What Is a Good Sleep Efficiency? Benchmarks, Formula, and What to Do Next
- The “3 A.M. Wake-Up”: Causes, Quick Fixes, and When to Look Deeper
References
- Hal Higdon — Post Marathon Recovery
- Polar — Post Marathon Recovery
- Brown F et al. — Compression Garments and Recovery from Exercise: A Meta-Analysis. (2017)
- Stedge HL & Armstrong K — The Effects of Intermittent Pneumatic Compression on the Reduction of Exercis... (2021)
- American Dietetic Association et al. — American College of Sports Medicine position stand. Nutrition and athletic pe... (2009)
- ACSM — Position Stand: Exercise and Fluid Replacement (2007)
- Finke et al. — [Medical emergencies during running events] (2023)
- Nieman et al. — Marathon training and immune function. (2007)
- Kwiecien et al. — The cold truth: the role of cryotherapy in the treatment of injury and recovery from exercise. (2021)
- Warhol et al. — Skeletal muscle injury and repair in marathon runners after competition. (1985)
- Hill et al. — Compression garments and recovery from exercise-induced muscle damage: a meta-analysis. (2014)
- Hal Higdon — Advanced Post Marathon Recovery